Endometriosis
Key points about endometriosis
- Endometriosis (kōpū whakatupu pūtautau) is a common condition where tissue similar to endometrial tissue, which should only be found in the uterus (womb), also grows outside the uterus, such as on ovaries or the bowel.
- Endometriosis affects up to 1 in 10 women and teenage girls.
- The cause of endometriosis is not fully known, but it often runs in families.
- The most common symptom of endometriosis is pelvic pain.
- Endometriosis can be very difficult to diagnose. The only sure way is by a surgical procedure called a laparoscopy.
- Treatment usually involves a combination of surgical, medical and self-management options.

Endometrial tissue is sensitive to hormone levels and changes as these fluctuate. In a normal menstrual cycle, hormones from your ovaries make the endometrial tissue grow. After a few weeks, if you do not get pregnant, these hormone levels decrease causing the endometrial tissue to shed and you have a period. In endometriosis, endometrial-like tissue, which has grown outside your uterus, also responds to the same hormones – the tissue grows and then bleeds. This can be very painful and is why, if you have endometriosis, you usually have pain leading up to and during your period. 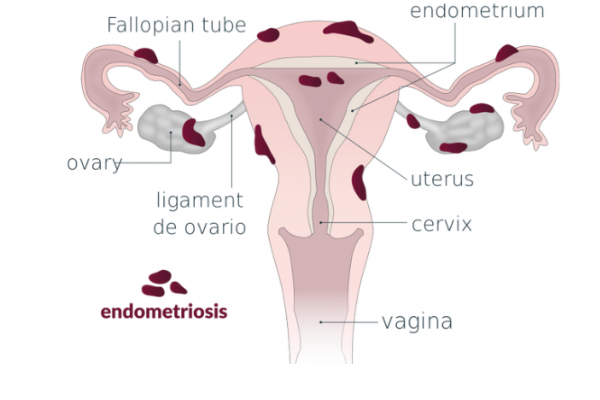
Image credit: Vega asensio Wikimedia Commons
Over time, the cycles of growth and break-down of the endometriosis tissue causes scarring, cysts and other damage on places such as the pelvic lining (peritoneum), ovaries and bowel. This is why early diagnosis and treatment are important to reduce possible complications, such as fertility problems.
In rare cases, endometriosis can be found in other parts of your body.
Video: What is endometriosis?
The most common symptom of endometriosis is pelvic pain. The pain is usually linked to your menstrual cycle. However, women with endometriosis may also experience pain at other times during the month.
For many women, the pain can be so severe it can prevent them from carrying out their normal daily activities. Some women with endometriosis may have no symptoms at all, which is less common.
Symptoms of endometriosis include:
- pain with periods (dysmenorrhoea)
- bowel problems, such as bloating, diarrhoea, constipation, pain with bowel movements (dyschezia), painful wind
- painful intercourse (dyspareunia)
- sub-fertility or infertility
- tiredness and low energy
- pain in other places such as the lower back or leg
- pain at other times, eg, with ovulation
- premenstrual syndrome (PMS)
- abnormal menstrual bleeding
- pain before or with urination, recurrent urinary tract infections (UTIs), or interstitial cystitis (inflammation of the bladder causing painful urination).
Looking at this factsheet on the symptoms of endometriosis(external link) may help you decide whether your symptoms are likely to be due to endometriosis. This visual tool(external link) may help you to put together the symptoms you are experiencing and help to focus any discussions you have with health professionals. If you experience symptoms regularly talk to your healthcare provider – you may need a referral to a gynaecologist.
Endometriosis can be very difficult to diagnose. The only sure way to diagnose endometriosis is by a surgical procedure called a laparoscopy. This is usually a straight-forward operation but like any operation, there are some risks. That is why tests will usually be done before surgery, such as:
- Physical examination and history taking: you will be asked about your periods and the pain associated with them. It can be useful to keep a diary(external link) of details about your periods or use an app to track them.
- Blood tests: there is no blood test which can diagnose endometriosis, but blood tests may be required to help rule out other conditions or before surgery.
- Ultrasound: the endometriosis tissue cannot be seen by ultrasound, but if there are endometriosis cysts then these can be seen. The results of scarring can also sometimes be seen by ultrasound.
- Laparoscopy: this procedure involves a small incision being made just below your tummy button. A lighted telescopic instrument called a laparoscope is inserted through the incision and the pelvic organs can be seen. This is done under a general anaesthetic by a specialist gynaecologist. During this procedure, tissue can be removed for testing, and endometriosis lesions can be removed, or organs that have become stuck together or to the pelvic wall can be separated.
Grades of endometriosis
Endometriosis is often classified as mild, moderate or severe, though different grading systems may be used.
- Mild – appears as small patches or surface lesions scattered around the pelvic cavity.
- Moderate – appears as larger widespread disease starting to infiltrate tissue and often found on the ovaries, uterosacral ligaments and pouch of Douglas.
- Severe – affects most of the pelvic organs, often with distortion of the anatomy and adhesions.
Grading like this can have limitations, eg, the extent of endometriosis is not generally related to the symptoms experienced.
Treatment for endometriosis involves a range of approaches, depending on your situation.
As the cause of endometriosis is still not understood, no particular treatment will provide a permanent cure. The most suitable treatment for you will depend on many factors, including:
- your age
- whether you plan to have children
- the severity of the symptoms
- the extent of endometriosis
- your preference.
Treatment usually involves a combination of:
- Self-care
- Medications
- Complementary therapies
- Surgical treatment.
To find the right treatment for your particular situation, a referral to a gynaecologist who has a special understanding and skill in treating pelvic pain and endometriosis is recommended.
All treatment options should be explored so that a long-term plan can be arranged. Unfortunately, endometriosis is known to recur, and repeat treatment procedures are sometimes necessary.
Healthy eating and keeping active are key ways to manage endometriosis. Some people with endometriosis have a sensitised bowel and find avoiding certain foods helpful. Others find complementary therapies helpful, especially in managing pain.
- Self-management FODMAP diet(external link) Endometriosis (NZ)
- Complementary therapies(external link) Endometriosis (NZ)
- Wellbeing, holistic and lifestyle(external link) Insight Endometriosis, NZ
Apps reviewed by Healthify
You may find it useful to look at some endometriosis apps.
Medications used in the management of endometriosis usually either relieve pain and inflammation or work on reducing the growth of the endometriosis itself and make your periods lighter. They are most useful for women who have mild endometriosis and who do not wish to get pregnant. Medications decrease the symptoms of endometriosis, but they do not cure it.
Pain-relieving medicines
A non-steroidal anti-inflammatory drug (NSAID) or paracetamol, used as required alone or in combination, is commonly used for pain relief. NSAIDs include ibuprofen, naproxen, celecoxib and mefenamic acid.
Tips about NSAIDs:
- They can help with pain and inflammation.
- There is no evidence that one particular NSAID is better than another.
- If the pain happens in cycles, start taking your NSAID the day before the pain is expected and continue taking it regularly while you have the pain (often 3–4 days).
- To better manage your pain, it is important to start pain relief medication early.
- NSAIDs can cause serious side effects such as stomach bleeding, increased risk of heart attacks and stroke and kidney problems. They are not suitable for everyone and are usually not recommended as a long-term treatment. Check with your doctor or pharmacist if NSAIDs are suitable for you.
If your pain is not relieved by using NSAIDs, other types of medication known as neuromodulators may be prescribed as they have pain relieving effects. You can read about them on the pain relief medications page under the headings of antidepressants and gabapentinoids. These medications are usually prescribed as part of a multidisciplinary team approach to care.
Hormone treatments
There are many different hormone treatments, most of which stop you from becoming pregnant. It is very important to discuss your plans about pregnancy with your doctor.
Progestogen-only treatment
Progestogens reduce oestrogen levels and stop ovulation. They thin the lining of the uterus (endometrium) making bleeding lighter, or stopping periods altogether. Progestogens are available in a variety of formulations.
| Progestogen-only treatments |
Progestogen-only oral contraceptive pill
|
Medroxyprogesterone acetate tablets (Provera)
|
Norethisterone tablets (Primolut N)
|
Medroxyprogesterone injection (Depo-Provera)
|
Intra-uterine device (IUD, Mirena)
|
Combined oral contraceptive pill (COCP)
The combined pill contains oestrogen and progestogen. It works by stopping ovulation and the hormone fluctuations associated with it, and in this way makes your periods lighter and less painful.
It is best to take the combined pill continuously, so you don't get a period. Take the hormone pills for 21 days and then go straight on to taking the hormone pills from a new packet. Do not take the 7 non-hormone pills. Repeat this every month. Read more about the combined oral contraceptive pill.
Goserelin (Zoladex)
This is given as an injection and is usually used when other medicines like the COCP or progestogen treatment can't be used or they did not work well enough.
Surgery is usually needed for more severe endometriosis, to reduce symptoms and improve the chance that your fertility will not be affected.
Laparoscopic surgery
Laparoscopic surgery as mentioned above is the only certain way to diagnose endometriosis. The aim is to remove all possible endometriosis lesions, cysts and adhesions, and restore normal anatomy. As with all surgery, there is an element of risk, which should be discussed with your surgeon.
Laparoscopic surgery for endometriosis is a specialised area of gynaecology and surgeons who perform these operations have usually had special training in this area.
Hysterectomy and oophorectomy
A hysterectomy is a procedure to remove the uterus and cervix and is sometimes recommended in severe cases of long-standing painful and extensive endometriosis for people who don't need future fertility.
Removal of one or both ovaries (oophorectomy) may be considered also if they have been damaged with cysts (endometrioma).
However, if both ovaries are removed, symptoms of menopause will usually be experienced immediately or very soon after surgery. Hormone replacement therapy (HRT) may be recommended and will depend on factors such as age, medical history and personal choice.
While symptoms of endometriosis are often eliminated or helped by hysterectomy, it does not cure the disease. To help prevent symptoms continuing, it is essential the endometriosis is removed at the same time as the hysterectomy.
Discuss surgical procedures thoroughly with your specialist. Sometimes symptoms persist even after major surgery and will require thorough review to find the cause.
Some people may find the use of complementary therapies helpful to manage the pain caused by endometriosis, but evidence for their use is lacking. Examples of complementary therapies include relaxation techniques such as breathing techniques, meditation, T'ai Chi and yoga. Tell your doctor if you are using complementary therapies. Together you can discuss any benefits of using complementary therapies and check interactions with your conventional medicine or treatment and any safety concerns. Read more about considerations if you are using complementary and alternative medicines.
Endometriosis New Zealand(external link)(external link)
Phone (03) 379 7959. Including a Facebook page to connect with hundreds of other’s affected by endometriosis, read about the latest research, check out support networks, patient partnering, useful links, resources.
Insight Endometriosis(external link)(external link)
Phone (07) 8555 123. Information and education to help women become expert patients, community support, personal appointments, information nights, coffee groups, phone support, Facebook page, newsletters.
About endometriosis(external link) Endometriosis, NZ
About endometriosis(external link) Insight Endometriosis, NZ
Endometriosis(external link)The Royal Australian and NZ Society of Obstetricians & Gynaecologists
Recent research about endometriosis(external link) Endometriosis, NZ
Endometriosis(external link) Mayo Clinic, US
Endometriosis – diagnosis and management(external link) BPAC, NZ
Endometriosis and pelvic pain(external link) Pelvic Pain Foundation of Australia
Raising Awareness tool for endometriosis (RATE)(external link) The Royal Australian and NZ Society of Obstetricians & Gynaecologists
Endometriosis factsheets(external link) Insight Endometriosis, NZ
Treating endometriosis(external link) The Royal Women’s Hospital Australia
Apps
Resources
Endometriosis(external link) RANZCOG, NZ, 2021
Endometriosis and pelvic pain(external link) Dr Susan Evans, Australia, 2012
Patient information for heavy periods and bleeding in between periods(external link) Auckland DHB, NZ, 2020
Chronic pelvic pain(external link) RANZCOG, 2016
Endometrial ablation(external link) RANZCOG, 2018
Symptom and Wellbeing tracker(external link) insight ENDOMETRIOSIS, NZ
Information guides from Insight ENDOMETRIOSIS, NZ
This is a link to the full page of guides(external link) or you can download individual ones by clicking on the links below.
Endometriosis(external link)
Adenomyosis(external link)
Diagnosing endometriosis in NZ(external link)
Surgery and hormonal management for endometriosis in NZ(external link)
Endometriosis pain and pain management(external link)
Complementary therapies and lifestyle changes for endometriosis(external link)
Mental wellbeing and self-care with endometriosis(external link)
Talking about endometriosis with people in your life(external link)
Self advocacy with medical professionals when you have endo(external link)
Fertility and endometriosis in New Zealand(external link)
Conditions related to endometriosis(external link)
Jigsaw of symptoms(external link)
Symptoms pain and food tracker(external link)
References
- The pharmacological management of endometriosis(external link) BPAC, 2013
- Chronic pelvic pain in women(external link) BPAC, 2015
- Hogg S, Vyas S. Endometriosis update(external link) Obstet Gynaecol Reprod Med. 2017; 28(3):61-69.
- Dunselman GAJ, Vermeulen N, Becker C, Calhaz-Jorge C, D’Hooghe T, De Bie B, et al. ESHRE guideline – management of women with endometriosis(external link) Hum Reprod. 2014;29(3):400–12
- Endometriosis(external link) Auckland region HealthPathways, NZ, 2020
- Endometriosis – diagnosis and management(external link) BPAC, NZ, 2021
Clinical resources
Raising awareness tool for endometriosis (RATE)(external link) Royal Australian College of Obstetricians and Gynaecologists, Australia, 2022
The Raising Awareness Tool for Endometriosis (RATE) is a quick-to-use electronic resource for health professionals and their patients to help identify and assess endometriosis – and endometriosis-associated symptoms – to reach a faster diagnosis and achieve more effective management of symptoms.
The pharmacological management of endometriosis(external link) BPAC, NZ, 2013
Latest news on endometriosis(external link) World Endometriosis Society, CA, 2021
Global forum for news and information about endometriosis(external link) Endometriosis.org
Insight Endometriosis(external link) supports people in Aotearoa New Zealand to make their own decisions about the treatment and management of their endometriosis through personal education appointments, informative seminars, in-person and online meet-ups, and providing evidence-based information on their website and through downloadable information sheets and factsheets.
Endometriosis NZ(external link) Provides a range of support for New Zealanders living with endometriosis.
The World Endometriosis Society(external link) (WES) convenes the World Congresses on Endometriosis (WCE). The 14th WCE takes place in Vancouver, Canada, 8–11 May 2020.
The World Endometriosis Research Foundation(external link) (WERF) is the global charity that fosters research in endometriosis to improve knowledge and treatments through international multi-centre research according to standardised protocols. WERF works with 62 centres in 25 countries.
Continuing professional development
eLearning
Endometriosis eLearning module(external link) Royal Australian College of Obstetricians and Gynaecologists, Australia
Podcast
Endometriosis - Anil Sharma(external link) Goodfellow Unit, NZ, 2019
Anil Sharma talks about the management of endometriosis in primary care. Anil is a private gynaecologist working in Auckland at Ascot Central and has special interests in endometriosis, abnormal uterine bleeding and urogynaecology.
Apps
Brochures
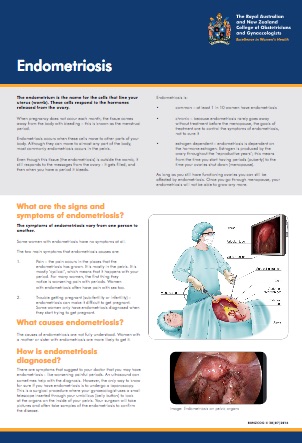
RANZCOG, NZ, 2021
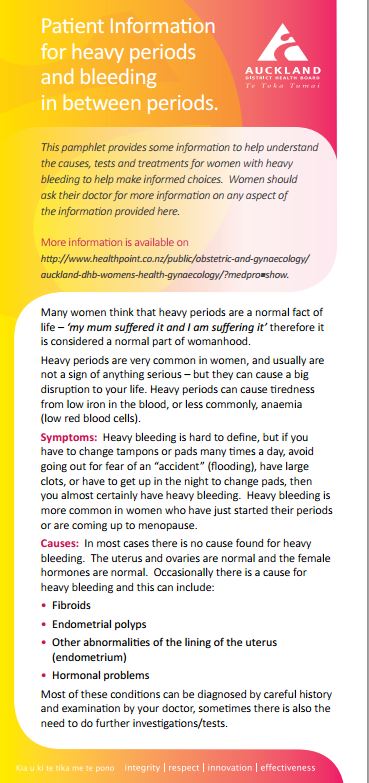
Auckland DHB, NZ, 2020
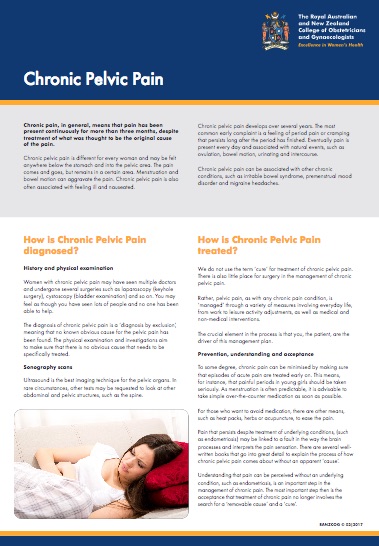
RANZCOG, 2016
Need help now?

![]()
![]()
Credits: Healthify editorial team. Healthify is brought to you by Health Navigator Charitable Trust.
Reviewed by: Dr Zoe LaHood, Senior House Officer, Hutt Valley DHB, NZ
Last reviewed:
Page last updated:
