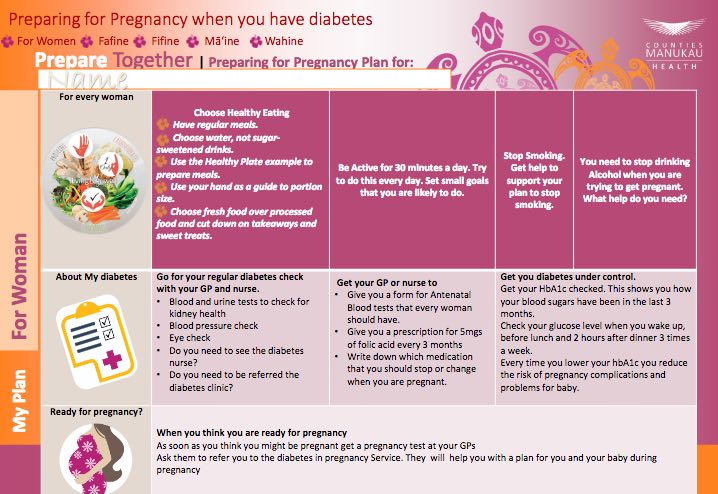
The best way to reduce the risks to you and your baby is to ensure your diabetes is well controlled before you become pregnant. Let your healthcare provider or diabetes specialist know 3–6 months before you start trying for a baby. They can refer you to a diabetes clinic for pre-pregnancy counselling and support. Pre-pregnancy counselling and planning have been shown to reduce the risk of poor outcomes.
Your blood glucose levels need to be closely monitored. You should be offered a blood test (HbA1c) every month. This measures the level of glucose in your blood. Continue using contraception and delay getting pregnant until your blood glucose is well controlled (HbA1c is under 48 mmol/mol or your personal target is met). However, not everybody can plan their pregnancy. If you have diabetes and think you might be pregnant, see your doctor as soon as you can.
Your healthcare team will review your medicines. If you are taking sulphonylurea to control your diabetes, this is likely to be stopped and replaced with insulin. Medicines such as statins or ACE inhibitors will also be stopped as they may cause harm to the development of your baby.
Folic acid
Women with diabetes should take a higher dose of 5 milligrams (mg) of folic acid each day while trying to get pregnant and until you are 12 weeks pregnant. Your doctor will have to prescribe this, as 5mg tablets are not available over-the-counter at the pharmacy.
Taking folic acid helps to prevent your baby from developing birth defects, such as spina bifida.(external link) Your doctor will also prescribe iodine 150 micrograms daily for you to take.
Other things you can do
- Eat a healthy balanced diet as guided by your dietitian.
- Stay active – aim for at least 30 minutes of exercise, such as walking or swimming, 5 or more days each week.
- Aim for a healthy body weight.
- Avoid alcohol, smoking and recreational drugs.
- Make sure your vaccinations are up to date.
- Visit your dentist and get checked for periodontal (gum) disease. If you have diabetes, you are at higher risk of gum disease and gum disease puts you at higher risk of adverse pregnancy outcomes.