Tubal ligation
Also called 'female sterilisation', 'permanent tubal contraception' or 'having your tubes tied'
Key points about tubal ligation
- Tubal ligation involves an operation which stops you getting pregnant.
- It's a small operation in which your fallopian tubes are removed, cut or blocked. This stops sperm from reaching an egg to fertilise it.
- It should only be considered when you're absolutely sure you do not want to have a child in the future.
- It's very reliable and in most cases will prevent pregnancy but it's not 100% effective and doesn't protect against sexually transmitted infections (STIs).
- The surgery is done under general anaesthetic with a simple laparoscopic (keyhole) procedure.

Tubal ligation is a surgical procedure where your fallopian tubes are removed from both sides, or closed off to stop sperm from reaching an egg to fertilise it. It’s also called ‘having your tubes tied’, ‘female sterilisation’ or 'permanent tubal contraception'. Because it’s permanent it’s important to be sure you don’t want children, or more children, before having it done.
The surgery doesn’t affect your ovaries, so you still continue to produce hormones and have menstrual periods afterwards. It also doesn’t affect the age when you’ll reach menopause.
During tubal ligation, the fallopian tubes can:
- be removed completely from both sides – currently this is the most common procedure
- be cut and have a section removed
- have a clip, band or ring placed around them.
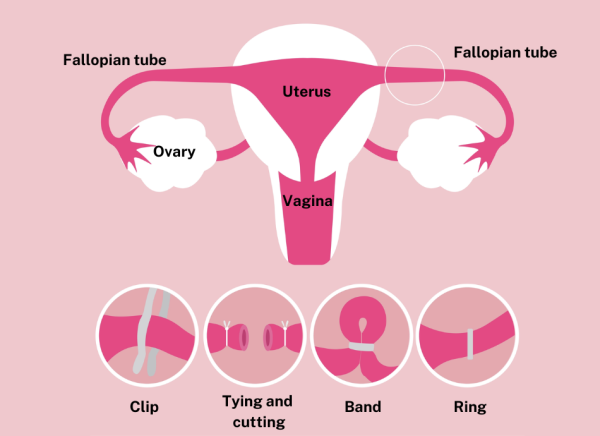
Image credit: Depositphotos (labels added)
There are 2 approaches to surgery – laparoscopy and mini-laparotomy. Your healthcare provider will discuss the options with you.
Laparoscopy
This is the most common surgical approach used for tubal ligation. It involves the following steps:
- Two small incisions (cuts) are made in your abdomen (tummy). A laparoscope (a long thin tube with a camera and light source at its tip) is inserted through one incision and surgical instruments are inserted through the other incision.
- The fallopian tubes are then able to be located and the procedure performed.
- The cuts in your abdomen are closed with steri-strips (small paper tapes) or small stitches.
Laparoscopic surgery is performed under a general anaesthetic. The procedure takes about 30 minutes, and you don't usually need to stay overnight in hospital.
Mini-laparotomy
Occasionally an 'open' surgical approach known as mini-laparotomy may be needed if the laparoscopic approach isn't suitable. This is now rare as it's safer to use long-acting reversible contraception instead. Mini-laparotomy is performed under general anaesthetic. A single incision of about 4 to 5 cm long is made, just above your pubic hair line. You will likely need to stay overnight in hospital.
What to expect afterwards
You may experience some or all of the following after your tubal ligation:
- Shoulder pain (referred pain from your abdomen)
- A sore throat after having a tube inserted during the surgery.
- Some bloating and cramping in your tummy (abdomen).
- Some discharge or bleeding from your vagina.
At the time of the operation you’ll be given advice about what to do and what not to do following your surgery.
General self-care:
- Take pain medication (eg, paracetamol) if you need it in the first few days.
- Keep your wound clean, dry and covered. Your healthcare team will tell you how often to change your dressing.
- Don’t go swimming, have a spa or a bath until the wound has healed.
- Stick to gentle exercise for a few days.
- Avoid lifting anything heavy for 3 weeks.
- You can have sex when you feel like it.
- You can return to work after a few days.
Contact your healthcare provider if you:
- have severe pain
- have heavy bleeding from your vagina, or the bleeding doesn’t settle after a day
- have a fever (high temperature)
- feel sick or vomit
- get an infection in your wound.
Read more about surgical wound care and wound infections.
Removing both tubes is very reliable and will usually prevent pregnancy. Very rarely an ectopic pregnancy may happen if a fertilised egg implants in the cut end of the tube.
If you have your tubes cut or blocked rather than removed completely, about 1 in 200 people may become pregnant. This may happen if:
- the fallopian tubes are not cut or blocked properly
- the cut ends grow back together
- the clips used to block the tubes migrate (move).
If pregnancy does occur after you have your tubes cut or blocked, there's a higher chance that it will be ectopic. This means that the pregnancy happens outside your uterus (womb), usually in your fallopian tubes, where the fetus can’t survive.
Advantages
- You don’t have to remember to take a pill every day.
- You would usually be asleep (under general anaesthetic) during the procedure.
- After the procedure is complete, it’s a private method of avoiding pregnancy as you don't have to take contraceptives.
- It doesn’t interfere with sex.
- Removal of the whole tube can slightly reduce your risk of ovarian cancer, which is why it's the standard procedure now. However, if it's not possible, then cutting and tying the tubal ends or occluding (blocking) the tubes is a good alternative.
Disadvantages
- Tubal ligation is intended to be permanent, so it’s a difficult procedure to reverse. You may regret having it done, especially if your circumstances change and you would like to have a baby.
- If your tubes are removed, that can't be reversed. In vitro fertilisation (IVF) would be required for any future pregnancy.
- Tubal ligation doesn't protect against sexually transmitted infections (STIs). Using condoms is the best way to prevent STIs.
- There are possible surgery-related complications – see below.
- You may not be eligible for public funding which would mean having to pay for the procedure yourself. Services may be prioritised based on clinical need.
Tubal ligation is a generally safe procedure with very few complications. Most people have no problems afterwards.
However, there is a small risk of:
- infection, bruising or bleeding at the operation site
- pelvic pain or pain in your abdomen (tummy)
- a possible reaction to the anaesthetic
- damage to organs, including your bowel, bladder, uterus, ovaries, blood vessels and nerves – but this is rare.
Contraception – your choice chart(external link) Sexual Wellbeing Aotearoa, NZ, 2024
Tubal ligation(external link) Protected and Proud, NZ
References
- New Zealand Aotearoa's guidance on contraception(external link) Ministry of Health, NZ, 2020
- Contraception – tubal ligation(external link) Better Health Channel, Australia
- Tubal ligation(external link) Protected and Proud, NZ
- Tubal ligation – discharge(external link) MedlinePlus, NIH, US, 2024
Need help now?

![]()
![]()
Credits: Healthify editorial team. Healthify is brought to you by Health Navigator Charitable Trust.
Reviewed by: Dr Jessica Dunning, Obstetrician and Gynaecologist, Te Toka Tumai Auckland and Auckland Gynaecology Group.
Last reviewed:
